





Home / 3D anatomy models / 3D anatomical models of pathologies and diseases / Chronic hydrocoele
Chronic hydrocoele




Chronic hydrocoele
 Download a PDF file Add to quotation - wish list
Download a PDF file Add to quotation - wish listProduct description: Chronic hydrocoele

Clinical History
An 80-year old male presented with haematemesis. He has a known history of alcoholic liver cirrhosis with oesophageal varices. On examination, he is noted to have multiple spider naevi, large volume abdominal ascites and a scrotal swelling. Transillumination of the swelling transmitted red light. He experienced another large volume haematemesis and died shortly after admission.
Pathology
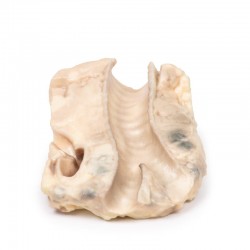
The specimen consists of a testis, tunica vaginalis and distal end of the spermatic cord. The testis and its surrounding layers have been bisected to display the cut surface. The tunica vaginalis is thickened and the enclosed cavity is distended. The testis is normal. This is an example of a chronic secondary communicated hydrocoele.
Further Information
A hydrocele is an accumulation of serous fluid between the parietal and visceral layers of the tunica vaginalis around the testes. Hydroceles can be described as communicating with the peritoneal cavity or noncommunicating with the peritoneal cavity. Communicating hydroceles develop due to failure of the processus vaginalis to close after the descent of the testes into the scrotum. These may present after birth as a congenital hydrocele or may present later in life due to increase in intra-abdominal pressure such a cardiac failure in this case. Non-communicating hydroceles are caused by imbalances in fluid secretion and reabsorption (e.g. orchitis, epididymitis), testicular tumour, physical trauma (e.g. hernia, testicular torsion) or defective lymphatic drainage (e.g. filariasis, elephantiasis). Patients present with a scrotal mass. The mass may be uni- or bilateral. Communicating hydroceles may be reducible and increase in size with raised intra-abdominal pressure. Non-communicating are usually nonreducible swellings. The swelling is usually non tender unless there is an underlying infection or torsion causing the hydrocele. Larger hydroceles may be cumbersome and cause erosion and skin infections on the scrotum. Diagnosis can be made on physical examination. Serous fluid allows the passage of light shined through the scrotum when examined: this is called transillumination. Ultrasound may be used to consolidate diagnosis and exclude other testicular pathology. Testicular cancer serum markers, such as alpha fetoprotein and B-HCG, may be taken to exclude testicular cancer. Many congenital hydroceles resolve spontaneously before the age of 2. If communicating hydroceles persist beyond 2 year they are surgically repaired due to the risk of developing incarcerated hernias. Surgical repair of communicating hydroceles in older patients may be offered if they are symptomatic. Treatment of the underlying aetiology of reactive hydrocele may cause them to resolve.
Inquiry
Related products














{kind=link}