




Home / 3D anatomy models / 3D anatomical models of the brain / Pituitary Adenoma
Pituitary Adenoma



Pituitary Adenoma
 Download a PDF file Add to quotation - wish list
Download a PDF file Add to quotation - wish listProduct description: Pituitary Adenoma

Clinical History
A 29-year old male presented with a 22 month history of headaches and blurred vision. Examination revealed a bi-temporal hemianopia and a left VIth nerve palsy. Skull X-ray showed erosion of most of the sphenoid body with some dorsum sellae and anterior clinoid process intact. Carotid angiography showed upward and lateral displacement of the anterior and middle cerebral arteries. Pneumoencephalography (a common imaging procedure used until the 1970s in which CSF is drained and replaced by air, oxygen or helium that acted as a contrast medium in X-ray examinations) showed upward displacement of the lateral and third ventricles from below. A craniotomy was performed but the patient died immediately afterwards
Pathology
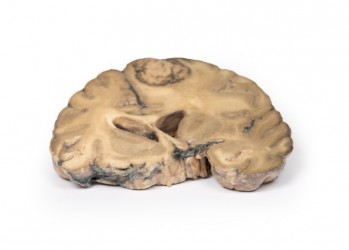
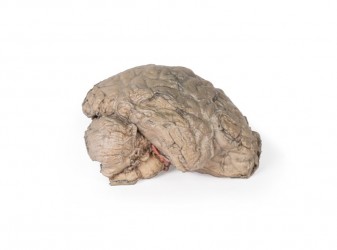
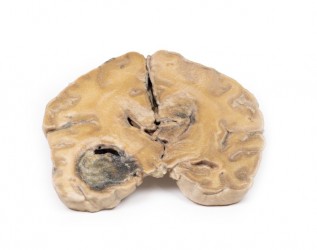
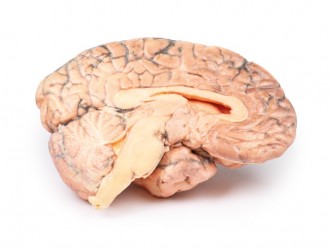
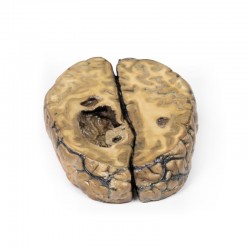
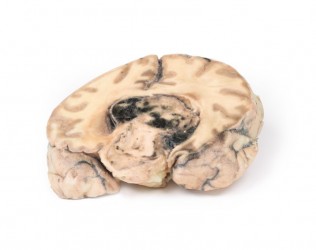
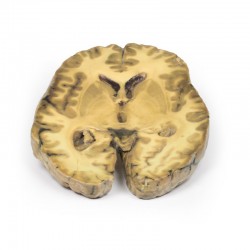
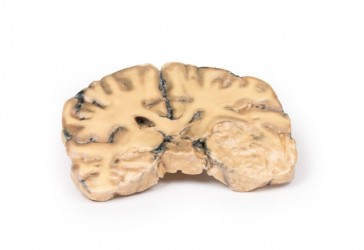
The brain specimen is sliced in the sagittal plane to the right of the falx cerebri, which remains in-situ. The pituitary gland has been completely replaced by a round tumour 4cm in maximum diameter. The tumour cut surface is pale brown and homogenous (except for an area of haemorrhage superiorly, likely caused by surgical trauma). The tumour has resulted in upward displacement of the midbrain. Tumour erosion has destroyed the sphenoid bone; thus, the sella turcica is enlarged (arrow). The optic chiasma is compressed by the tumour. Histologically, this tumour was a chromophobe adenoma arising from the anterior pituitary.








{kind=link}